Writing this from Appalachia, and having grown up in this community, I have seen how drugs affect every single part of our day-to-day life. Virtually every family has been affected by the drug epidemic. This epidemic, much like the coronavirus pandemic, is a worldwide issue. Different countries have taken a multitude of approaches in dealing with this problem. Some European countries have more lax drug laws, and other countries, such as Singapore, hand out the death penalty for large-scale trafficking of illicit substances. There might not be a perfect solution to this problem, but the system we have in place today has proven to be ineffective.
Drug use has been a part of the world for centuries. Decriminalization of every illicit drug in America, as well as promoting the epidemic as a mental health issue, would remove the stigma associated with drug use and promote a better alternative than overcrowding prisons. Unfortunately, thousands are arrested for simple drug possession, and instead of receiving treatment for their disease, they are confined to a prison cell. Without the necessary tools to help with their addiction, and now an arrest record, the endless cycle of drugs and incarceration will continue. This paper will serve as an analysis of how America fumbled its drug policies and an in-depth look at how other countries are combating the drug epidemic as a mental health issue. Furthermore, this paper will describe what decriminalization entails and the following pros and cons. There may not be a perfect solution, but criminalizing a mental health issue is not the way to recovery. First, we will examine the United States’ failed attempt at prohibiting alcohol.
I. Prohibition of Alcohol
On November 18, 1918, prior to the ratification of the Eighteenth Amendment, the U.S. Congress passed the temporary Wartime Prohibition Act, which banned the sale of alcoholic beverages having an alcohol content of greater than 1.28%.[1] This Act, which had been intended to save grain for the war effort, was passed after the armistice ending World War I was signed on November 11, 1918.[2] The Act took effect June 30, 1919, with July 1 becoming known as the “Thirsty First.”[3]
Kansas became the first state to outlaw alcoholic beverages in 1881 and quickly amended it to its Constitution.[4] Carrie Nation, a prohibition activist at the time, was arrested, fined, and incarcerated on multiple occasions. Nation attempted to individually enforce the state’s ban on alcohol consumption. Nation recruited ladies into the Carrie Nation Prohibition Group, which she also led. “While Nation’s vigilante techniques were rare, other activists enforced the dry cause by entering saloons, singing, praying, and urging saloonkeepers to stop selling alcohol.”[5] “Other dry states, especially those in the South, enacted prohibition legislation, as did individual counties within a state.”[6]
Court cases also debated the subject of prohibition. While some cases ruled in opposition to prohibition, the general tendency was to support it. In Mulger v. Kansas,[7] Justice Harlan commented: “We cannot shut out of view the fact, within the knowledge of all, that the public health, the public morals, and the public safety, may be endangered by the general use of intoxicating drinks; that the idleness, disorder, pauperism, and crime existing in the country, are, in some degree . . . . traceable to this evil.”[8] In support of prohibition, the court in Crowley v. Christensen,[9] remarked: “The statistics of every state show a greater amount of crime and misery attributable to the use of ardent spirits obtained at these retail liquor saloons than to any other source.”[10]
Prohibition began on January 17, 1920, when the Volstead Act went into effect. A total of 1,520 Federal Prohibition agents (police) were tasked with enforcement.[11] Following the ban, criminal gangs gained control of the beer and liquor supply in many cities. By the late 1920s, a new opposition to Prohibition emerged nationwide. Critics attacked the policy as causing crime, lowering local revenues, and imposing “rural” Protestant religious values on “urban” America. Prohibition ended with the ratification of the Twenty-First Amendment, which repealed the Eighteenth Amendment on December 5, 1933, though prohibition continued in some states. To date, this is the only time in American history in which a constitutional amendment was passed for the purpose of repealing another.[12]
Prohibition was ultimately a failure. Over the course of its inception, it failed to decrease the overall consumption of liquor; it also failed to reduce taxpayer burden, the prison population, and public corruption. The Eighteenth Amendment ultimately increased all of these things.[13] "According to Mark Thornton of Cato and Auburn University, “(c)rime in general increased some 24% in the 30 largest cities between 1920 and 1921, while the homicide rate during this time was 78% higher than in the decade preceding it.”[14] “Naturally, an increase in the rate of crime corresponded with an increase in money spent on enforcement, and an increase in the number of inmates processed throughout the prison system.”[15] Lessons were not learned from the failures of prohibition when early and modern drug laws were enacted.
II. Early Drug Laws
The modern drug war was launched by a single event that took place over 100 years ago.[16] President Woodrow Wilson signed the Harrison Narcotics Act of 1914 and committed the federal government to combating the domestic drug trade. The Harrison Act aimed to ban nonmedical use of opiates and cocaine.[17] “Together with the Marihuana Tax Act of 1937, it federalized what till then had been a state-by-state skirmish against recreational drugs.”[18] These laws were considered important at the time, but the laws arrived too late to teach us why anti-drug laws took the rise. “The Harrison Act became law only after thirty-five states and territories had banned opium and forty-six had banned cocaine and Congress passed the Marihuana Tax Act only after all fifty states and territories had banned marijuana.”[19]
The Act also marked the beginning of the criminalization of addiction and the American black market for drugs. Just as Prohibition led to bootleggers, this Act led to drug traffickers. Within five years, the Rainey Committee, a Special Committee on Investigation appointed by Secretary of the Treasury and led by Congressman T. Rainey, reported in June 1919 that drugs were being smuggled into the country by sea, and across the Mexican and Canadian borders by nationally established organizations. “The United States consumed 470,000 pounds of opium annually, compared to 17,000 pounds in both France and Germany.[20] The Monthly Summary of Foreign Commerce of the United States recorded that in the seven months to January 1920, 528,635 pounds of opium was imported, compared to 74,650 pounds in the same period in 1919.”[21]
In 1969, Richard Nixon announced that the Attorney General was preparing a comprehensive new measure to more effectively meet the narcotic and dangerous drug problems at the federal level by combining all existing federal laws into a single new statute.[22] As a result, the Controlled Substances Act was created and combined existing federal drug laws and expanded their scope. Furthermore, the Controlled Substances Act changed the nature of federal drug law policies and expanded federal law enforcement’s authority on controlled substances.[23] There are five different schedules of controlled substances, numbered I–V. The Controlled Substances Act describes the schedules based on three factors:
-
Potential for abuse: How likely is this drug to be abused?
-
Accepted medical use: Is this drug used as a treatment in the United States?
-
Safety and potential for addiction: Is this drug safe? How likely is this drug to cause addiction? What kinds of addiction?[24]
Schedule I drugs are designated as having a high possibility of abuse, having no accepted medical use, being unsafe, and having a high potential to be addicting. Marijuana, MDMA, and Psilocybin, to name a few, are designated Schedule I drugs. The Controlled Substances Act placed a moratorium on research with Schedule I substances, hampering medical research for decades. Only recently has research with these compounds been resurrected. “In 2018, the FDA assigned psilocybin and MDMA, both Schedule I drugs, ‘Breakthrough Treatment’ designations.”[25] “This begs the question: How could these drugs simultaneously be breakthrough treatments and have no medical value?”[26] The Controlled Substances Act bans the study of substances that could provide valid medical or therapeutic use, which halted the study of marijuana for decades.
The failure of the Controlled Substances Act has become abundantly clear by looking at it through the eyes of the criminal rather than through the eyes of an individual in need of medical treatment. There is a lack of evidence demonstrating that overall, U.S. drug use has decreased since the passage of the Controlled Substances Act. At the same time, the U.S. prison system has burgeoned to the largest in the world, with around 20% of those incarcerated solely for drug possession.[27] Drug offenses still account for the incarceration of almost 400,000 people, and drug convictions remain a defining feature of the federal prison system.[28] Police still make over one million drug possession arrests each year, many of which lead to prison sentences.[29] Drug arrests continue to give residents of over-policed communities criminal records that ultimately hurt their employment opportunities and increase the likelihood of longer sentences for any future offenses.[30]
III. War on Drugs
The War on Drugs in America has been forged by laws that could be argued were beyond Congress’s powers to enact. The Supreme Court has given Congress a long leash with their interpretation of the Commerce Clause. In Gonzales v. Raich,[31] Angel Raich, and Diane Monson (plaintiffs) were California residents who both legally used marijuana to treat legitimate medical issues. Despite receiving approval from California state officials, federal agents seized and destroyed Raich’s marijuana plants.[32] Raich brought this suit against Alberto Gonzales, Attorney General of the United States (defendant), seeking injunctive and declaratory relief prohibiting the enforcement of the Controlled Substances Act. The Court of Appeals in California ruled that the Controlled Substances Act was an invalid exercise of Congress’s Commerce Clause power, and Gonzales appealed to the United States Supreme Court.[33]
Justice Stevens held, writing for the majority, that Raich’s activity of growing marijuana for home use can be seen rationally as having a substantial effect on interstate commerce because there is an established, albeit illegal, interstate market for marijuana. Therefore, the Controlled Substances Act is a valid exercise of Congress’s Commerce Clause power because Congress acted rationally in determining that growing marijuana was an economic activity with a substantial effect on interstate commerce.[34]
Justice Thomas made the correct assertion in his dissent that Raich’s activities in growing marijuana for home are is not properly categorized as “commerce.” “The marijuana in question was never bought or sold; never crossed state lines; and had no demonstrable effect on the national marijuana market.”[35] “Congress has broad authority to regulate local activities that have a substantial effect on interstate commerce, but this provision, even when amplified by the Necessary and Proper Clause, has limits.”[36] Congress did not demonstrate that regulation of medical marijuana is necessary to combat the interstate drug trade. Accordingly, Congress’s actions violated the Tenth Amendment.[37] Although it took a constitutional amendment to allow Congress to prohibit alcohol nationwide, the prohibition of illicit substances took place without any amendment.
In June 1971, Nixon officially declared a “War on Drugs,” stating that drug abuse was “public enemy number one.”[38] A rise in recreational drug use in the 1960s likely led to Nixon’s focus on targeting some types of substance abuse. As part of the War on Drugs initiative, Nixon increased federal funding for drug-control agencies and proposed strict measures, such as mandatory prison sentencing, for drug crimes.[39] Nixon went on to create the Drug Enforcement Administration (DEA) in 1973. This agency is a special police force committed to targeting illegal drug use and smuggling in the United States.[40] At the start, the DEA was given 1,470 special agents and a budget of less than $75 million. Today, the agency has nearly 5,000 agents and a budget of $2.03 billion.[41]
In 1986, the U.S. Congress passed laws that created a 100 to 1 sentencing disparity for the trafficking or possession of crack when compared to penalties for trafficking of powder cocaine, which had been widely criticized as discriminatory against minorities, mostly African Americans, who were more likely to use crack cocaine other than powder cocaine.[42] “This 100:1 ratio had been required under federal law since 1986, and persons convicted in federal court of possession of five grams of crack cocaine received a minimum mandatory sentence of five years in federal prison.”[43] On the other hand, possession of 500 grams of powder cocaine carries the same sentence. In 2010, the Fair Sentencing Act cut the sentencing disparity to 18:1.[44] According to Human Rights Watch; crime statistics show that African Americans are far more likely to be arrested for drug crimes, and received much stiffer penalties and sentences.[45]
In 1998, statistics showed racial disparities regarding arrests and sentencing. African American drug users comprised 35% of drug arrests, 55% of convictions, and 74% of people sent to prison for drug possession crimes.[46] “Nationwide, African Americans were sent to state prisons for drug offenses thirteen times more often than other races, even though they constituted only 13% of regular drug users.”[47] Anti-drug legislation over time has also displayed an apparent racial bias. University of Minnesota professor and social justice author Michael Torry writes, “The War on Drugs foreseeably and unnecessarily blighted the lives of hundreds and thousands of young disadvantaged black Americans and undermined decades of effort to improve the life chances of members of the urban black underclass.”[48]
The War on Drugs is ultimately an unwinnable war that has cost taxpayers billions of dollars while locking up countless individuals for simple possession. Decriminalization is a way to combat drug use, not through the judicial system, but by viewing drug use as a mental health issue. Unfortunately, the issue is too complex to be solved overnight; however, by learning from countries that have used decriminalization, the United States can stop the war on drugs and help substance abuse users get the help they need without looking through the bars of a prison cell.
IV. Drug Addiction as a Mental Illness
Addiction is defined as a disease by most medical associations, including the American Medical Association and the American Society of Addiction Medicine. Like diabetes, cancer, and heart disease, addiction is caused by a combination of behavioral, psychological, environmental, and biological factors.[49] Genetic risk factors account for about half of the likelihood that an individual will develop addiction. “Addiction involves changes in the functioning of the brain and body due to persistent use of nicotine, alcohol, and/or other substances.”[50]
The consequences of untreated addiction often include other physical and mental health disorders that require medical attention. In addition, if left untreated over time, addiction becomes more severe, disabling, and potentially life-threatening.[51]
Substance abuse can change the brain. For example, there is pleasure when basic needs such as hunger, thirst, and sex are satisfied. In most cases, these feelings of pleasure are caused by the release of certain chemicals in the brain, which reinforce these life-sustaining functions by incentivizing the individual to repeat the behaviors that produce those rewarding feelings (eating, drinking and sex).[52] Most addictive substances cause the brain to release high levels of these same chemicals that are associated with natural pleasure or reward.[53]
Over time, the continued release of these chemicals causes changes in the brain systems involved in reward, motivation, and memory. The brain tries to get back to a balanced state by minimizing the effects will essentially bring the substance abuser back to a normal state. As a result, a person may need to use increasing amounts of the substance just to feel closer to normal. The individual may experience intense desires or cravings for the substance and will continue to use it despite harmful or dangerous consequences. Additionally, a person may prefer the substance to other healthy pleasures and may lose interest in normal life activities. In the most chronic form of the disease, a severe substance use disorder can cause a person to stop caring about their own or others’ well-being or survival.[54]
These changes in the brain can remain for a long time, even after the person stops using substances.[55] It is believed that these changes may leave those with addiction vulnerable to physical and environmental cues that they associate with substance use, also known as triggers, which can increase their risk of relapse. “Physical addiction appears to occur when repeated use of a drug changes the way your brain feels pleasure.”[56] “The addicting drug causes physical changes to some nerve cells (neurons) in your brain.”[57] “Neurons use chemicals called neurotransmitters to communicate and these changes can remain long after you stop using the drug.”[58]
The beginning stages of someone’s decision to use illicit substances are based largely on a person’s free or conscious choice, but this choice can often be influenced by the circumstances of where they live and the environment around them. “Certain factors, such as a family history of addiction, trauma, or inadequately treated mental health disorders such as depression and anxiety, may make some people more susceptible to substance use disorders than others.”[59] Once the brain has been changed by addiction, that choice or willpower becomes impaired, and the substance takes priority over the individual, and their livelihood.[60]
Some people are under the assumption that addiction is not a mental health issue because it is caused by the individual’s choice to use the substance and, therefore, they should have to deal with those consequences. “While the first use (or early-stage use) may be by choice, once the brain has been changed by addiction, most experts believe that the person loses control of their behavior.”[61] “Choice does not determine whether something is a disease.” “Heart disease, diabetes and some forms of cancer involve personal choices like diet, exercise, sun exposure, etc. A disease is what happens in the body as a result of those choices.”[62] Just because choosing to eat three doughnuts every day, survive off fast food, and live a sedentary lifestyle does not hurt you in the short term, it is still considered an addiction. “Some studies have suggested that sugar is as addictive as Cocaine.”[63] People often enjoy the dopamine release that sugar brings. But due to the addictive nature of sugar, long-term health effects such as obesity and diabetes are a risk of sugar overindulgence. The stigma of the substance abuse user should be viewed in a similar light with less policing and more treatment facilities.
Individuals make poor choices that hurt their health on a daily basis. Decriminalization of drug possession or drug use should be viewed the same way we view other ailments that involve personal choices. Our society will help the individual that is addicted to sugar and drinks twenty cans of coca cola per day, knowing it is ultimately killing them, by providing them medicine and healthcare. Likewise, substance abuse should be given that same type of treatment.
V. Incarceration and Substance Abuse Disorders
The substantial prison population in the United States is strongly connected to drug-related offenses. “While the exact rates of inmates with substance use disorders (SUD’s) is difficult to measure, some research shows that an estimated 65% percent of the United States prison population has an active substance abuse disorder.” “Another 20% percent did not meet the official criteria for a substance abuse disorder, but were under the influence of drugs or alcohol at the time of their crime.”[64]
Decades of scientific studies show that providing comprehensive substance use treatment to criminal offenders while incarcerated works, reducing both drug use and crime after an inmate returns to the community.[65] Treatment while in jail or prison is critical to reducing overall crime and other drug-related societal burdens—such as lost job productivity, family disintegration, and a continual return to jail or prison, known as recidivism. Inadequate treatment while incarcerated also contributes to overdoses and deaths when inmates leave the prison system.[66] The days and weeks following release from incarceration are also a particularly high-risk period for overdose death.[67] A seminal study in Washington State found that, in the two weeks following their release, people who had been incarcerated in state prisons were 129 times more likely to die from an overdose compared to the general public.[68] A recent study from North Carolina state prisons corroborated this heightened risk, finding that formerly incarcerated people were 40 times more likely to die of an opioid overdose two weeks post-release.[69]
To be effective for this population, treatment must begin in prison and be sustained after release through participation in community treatment programs. By engaging in a continuing therapeutic process, people can learn how to avoid relapse and withdraw from a life of crime. However, only a small percentage of those who need treatment while behind bars actually receive it, and often the treatment provided is inadequate.[70] However, if individuals charged with simple possession, or even dealing small quantities to support their habit, were treated like those with a mental health issue, those individuals’ would have a better chance to win their own war with drugs.
VI. What is Drug Decriminalization?
Drug decriminalization is the elimination of criminal charges for drug possession and individual use, possession of equipment used to consume drugs and low-level drug sales.[71] Decriminalization is the elimination of criminal penalties for an activity, while legalization eliminates all penalties. In places where drugs are decriminalized, individuals may face civil penalties for the use or possession of a drug (e.g., fines or required counseling) but will not receive criminal charges, which can lead to incarceration and a criminal record.[72]
There have been proponents of full legalization. Some say legalization would be a way for drugs to be more regulated. First, full regulation would help with the toxicity levels of the drugs themselves. For drug dealers to make more money, they often cut their products with other substances, such as fentanyl, that make their drugs even far more deadly. Also, the government could bring in tax revenue from a legalized market. Similar to how states are benefiting from the legalization of marijuana.[73]
As with most positives in life, there is generally negativity hiding behind the corner. A con of full legalization is that it could lead to more people experimenting with drugs. Others warn that it could send the wrong message to the younger generation that it would be more socially acceptable to use drugs and give the impression that drugs are safe to consume.[74] Decriminalization is a softer approach to the drug epidemic than full legalization. We need to model our structure after the benefits Portugal and Switzerland have implemented and start to create a system that destigmatizes drug users while still punishing the large-scale drug traffickers.
VII. Portugal’s Strategy
Portugal has long been seen as the example of what decriminalization can like on a large scale. On July 1, 2001, a nationwide law in Portugal took effect that decriminalized all drugs. Under the new legal framework, all drugs were “decriminalized,” not “legalized.” “Thus, drug possession for personal use and drug usage itself are still legally prohibited, but violations of those prohibitions are deemed to be exclusively administrative violations and are removed completely from the criminal realm.”[75] Drug trafficking continues to be prosecuted as a criminal offense.[76]
Interviews with Portuguese political officials and drug policy experts confirm that they did not embrace decriminalization despite their belief that it would lead to increased usage. Rather, they embraced decriminalization as the best option for minimizing all drug-related problems, including addiction:
“Decriminalization is not expected to increase the amount of drugs available or the use of new types of drugs. However, there is a general belief that decriminalization increases the need for prevention, for example, to communicate to the public that decriminalization does not condone drug use. . . . There is a consensus that decriminalization, by destigmatizing drug use, will bring a higher proportion of users into treatment, thereby increasing the need for treatment.”[77]
The Institute on Drugs and Drug Addiction is in charge of overseeing the drug policy. It continues to define its core mission, and the core purpose of the decriminalization law, as follows:
“This law reinforces the resources in the context of demand reduction by sending to treatment drug addicts and [includes] those that are not addicts but need a specialized intervention. With this Law, we expect to contribute to the resolution of the problem in an integrated and constructive way, looking at the drug addict as a sick person, who nevertheless must be responsible for a behavior that is still considered an offense in Portugal.”[78]
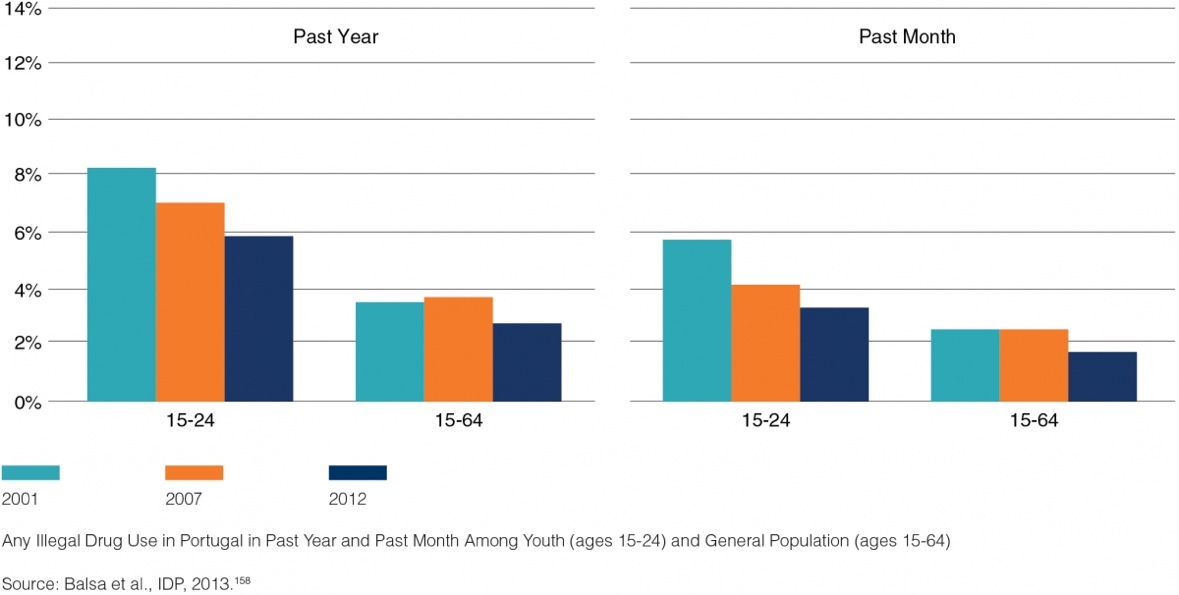
The following graph shows illegal drug use in Portugal before and after decriminalization.

VII. Switzerland’s Strategy and the Four-Pillar Policy
Swiss drug policy aims to reduce drug use and its negative consequences for users and society. It is based on the four pillars of prevention, therapy, harm reduction and repression. The revision of the Narcotics Act in 2008 enshrined the four-pillar drug policy in law, and the verbiage comes straight from the Narcotics Act.[79]
A. Pillar One: Prevention
This pillar includes measures for general health promotion that intend to strengthen individual health resources and prevent addiction problems.[80] On the other hand, it subsumes measures for behavioral and situational prevention that concern people’s health behavior or that are specifically geared towards issues with addiction which aim at preventing the emergence of risk behavior as far as possible. Early detection facilitates the earlier recognition of behavior that could lead to health or social problems or addiction.[81]
B. Pillar Two: Therapy and Counseling
Measures in the area of treatment are aimed at people who are addicted and who would like to reduce their consumption, as well as measures aimed at their relatives.[82] Counseling or treatment intends to support people in regaining control over their addiction or even to enable them to make a sustainable exit from addiction.[83] The aim of therapy and counseling is to improve the quality of life and the physical and psychological condition of those affected, as well as their social and professional integration.[84]
C. Pillar Three: Harm Reduction and Risk Minimization
Measures in the area of harm reduction aim to stabilize the state of health of those affected, maintain their social integration or facilitate reintegration, or offer them survival assistance, for example, by switching to less risky or less harmful behaviors.[85] Harm reduction aims to preserve the quality of life of those affected, so that they can lead a qualitatively good and, as far as possible, self-determined life despite current risky and addictive behavior, and later pave the way for therapy and withdrawal.[86]
D. Pillar Four: Regulation and Enforcement
The main goal of regulating alcohol, drugs, tobacco, medicines, or gambling is to protect people’s health. In the area of legal substances and behaviors, regulation includes government interventions aimed at limiting the accessibility and availability as well as the attractiveness of psychoactive substances or certain behaviors such as gambling (e.g., advertising restrictions, limiting sales hours, age restrictions). Finally, enforcement refers to the implementation of the existing legal framework.[87]
“The multi-pronged approach included some controversial measures — such as legalized drug consumption rooms and heroin-assisted treatment facilities — but ultimately, the statistics show it has been successful.”[88]
“Over the past two decades, the number of opioid-related deaths in Switzerland has decreased by 64%. The number of new HIV infections also dropped significantly.”[89] “In 1986, more than 3,000 people tested positive for HIV in Switzerland. In 2017, there were fewer than 500 new positive tests in a country of 8.4 million.”[90] Switzerland began mandatory Hepatitis C reporting in 1988, and the number of reported cases peaked between 1999 and 2002, declining since then."[91]
VIII. Oregon Ballot Measure 110
On February 1, 2021, Oregon became the first state in the U.S. to decriminalize the possession of small quantities of all illicit drugs, following the passing of Oregon Ballot Measure 110 in November 2020.[92]
Like Oregon, one of the central aspects of Portugal’s policy is the establishment of free treatment facilities along with information campaigns about the harms of drug use and needle exchange programs. In addition, individuals found with drugs on their person are charged with an administrative offense that requires them to appear before a committee where they are offered treatment or a small fine.[93]
Interpretations of the drug use data in Portugal vary widely depending on the metrics used. However, a collation of figures from the Transformation Drug Policy Foundation found that decriminalization, on the whole, was not associated with a rise in drug usage. Drug use rates in Portugal are now below the European average for cocaine, methamphetamine, and amphetamines.[94]
With nearly twenty years of data and documentation to assess the success of the policy, it is unsurprising that Oregon’s Measure 110 was largely inspired by Portugal’s wide body of research. It has shown a lack of relationship between the severity of drug laws and rates of drug usage. The studies focusing on drug use amongst adolescents are particularly reassuring.
Tracking the drug use of adolescents (ages 15 to 34) over time in Portugal has shown a steady decline in the use of cocaine, amphetamines, and MDMA between 2007 and 2012. More generally, continuous drug usage (relating to individuals who use drugs regularly) has decreased since decriminalization, and these results certainly do not constitute a surge in drug use.[95]
By moving away from criminalizing and imprisoning people who use drugs, the profile of the prison population has changed. “In 2001, over 40% of the sentenced Portuguese prison population were held for drug offences, considerably above the European average, and 70% of reported crime was associated with drugs.”[96] While the European average has gradually risen over the past twenty years (from 14 to 18%), the proportion of people sentenced for drug offences in Portuguese prisons has fallen dramatically to 15.7% in 2019 — now below the European average.[97] Oregon will need more data in order to determine if its results will mimic or surpass Portugal’s. However, realizing its drug policies were failing and having the courage to make a drastic change should give hope to other states that there are options other than criminalization.
IX. Conclusion
Most Americans have used an illicit drug at one point in their lives. Do you believe your husband, wife, son, or daughter should be thrown in jail for using an illicit substance and stigmatized as a drug user for the remainder of their lives? Drug decriminalization would drastically reduce the number of individuals arrested, incarcerated, and destigmatize the substance abuse issue. In addition, destigmatizing can revise the current law enforcement incentive structure and redirect those resources to prevent serious and violent crimes.
Drugs and drug use will never go away. It will be a part of our lives for the foreseeable future. The war on drugs has failed, and a new approach is needed. Drug addiction already has a stigma attached to it. “People are scared to get help, out of fear of what others might think.”[98] They will continue using drugs just to feel “better” or “normal.” This is part of the addiction cycle. The body becomes dependent on drugs to function normally. Drug addicts are not bad people; they are afflicted by a chronic mental health disease.[99] “Therefore, professional treatment is an important step in ensuring they get the help they need to break the cycle of addiction.”[100]
Mental health issues, such as anxiety or depression, have never been more in the spotlight than they are today. Professional athletes, whom people view as being mentally tough, are coming out and identifying their own mental health issues. Decriminalization is a way to bring substance abuse into the spotlight and treat it the same way we view any other mental health issue. A quote best said by the architect of Portugal’s decriminalization policy: “It’s very difficult to identify a causal link between decriminalization by itself and the positive tendencies we’ve seen. . . It’s a total package. The biggest effect has been to all the stigma of drug addiction to fall, to let people speak clearly and to pursue professional help without fear.”[101]
William D. Miller, Pretty Bubbles in the Air: America in 1919, (Univ. of Ill. Press 2017).
Id.
Id. at 151.
Prohibition, Kan. Hist. Soc’y, (Nov. 2001), https://www.kshs.org/kansapedia/prohibition/14523.
Carry A. Nation: The Famous and Original Bar Room Smasher, Kan. Hist. Soc’y, (Nov. 1, 2002).
Id.
Mulger v. Kansas, 123 U.S. 623 (1887).
Id. at 662.
Crowley v. Christensen, 137 U.S. 86 (1890).
Id. at 91.
Nation Voted Dry, 38 States Adopt the Amendment / Prohibition Map of the United States at 4, N.Y. Times (Jan. 17, 1919).
Margaret Sands Orchowski, The Law that Changed the Face of America: The Immigration and Nationality Act of 1965, 32 (Rowman & Littlefield).
Tarnell Brown, A Brief Look at Why Prohibition Laws Don’t Work (Aug. 26, 2020), https://www.econlib.org/a-brief-look-at-why-prohibition-laws-dont-work/.
Id.
Id.
A History of the Drug War, Drug Pol’y Org. (last visited Mar. 2023), https://drugpolicy.org/issues/brief-history-drug-war.
George Fisher, The Drug Wat at 100, Stan. L. Sch. (Dec. 19, 2014), https://law.stanford.edu/2014/12/19/the-drug-war-at-100/.
Id.
Id.
Harrison Narcotics Tax Act (1914), Drug Reform Coordination Network, https://www.druglibrary.org/schaffer/library/studies/cu/cu8.html.
The Pharmaceutical era, 53 (Mar. 10, 2001)
State and Local Task Forces, U.S. Dep’t of Just.: Drug Enf’t Agency (July 17, 2018), https://www.dea.gov/operations/state-and-local-task-forces.
National Commission on Marihuana and Drug Abuse, Drug Use In America: Problem In Perspective, Second Rep. of the National Commission on Marihuana and Drug Abuse (1973).
After 50 Years of Failure, It’s Time to Rethink the Controlled Substance Act, Students for Sensible Drug Policy, (Dec. 17, 2020) ssdp.org/blog/opinion-piece-after-50-years-of-failure-its-time-to-rethink-the-controlled-substances-act/.
Id.
Michelle Alexander. The New Jim Crow: Mass Incarceration in the Age of Colorblindness, N. Y.: The New Press 6, 2010.
Wendy Sawyer & Peter Wagner, Mass Incarceration: The Whole Pie 2022, Prison Pol’y Initiative (Mar. 14, 2022), https://www.prisonpolicy.org/reports/pie2023.html.
Id.
Id.
Gonzalez v. Raich, 545 U.S. 1 (2005).
Id. at 40.
Id.
Id. at 41.
Id. at 58.
Id. at 58-60.
War on Drugs, The Glob. Commi’n on Drug Pol’y, 24 (June 2011), file:///C:/Users/ASL/Downloads/global-commission-report-english-20110624.pdf.
Id.
Id.
Thirty Years of America’s Drug War, PBS: Frontline (Feb. 24, 2011), https://www.pbs.org/wgbh/pages/frontline/shows/drugs/cron/.
Id.
Alan Elsner, Gates of Injustice: The Crisis in America’s Prisons, (Saddle River, New Jersey: Financial Times Prentice Hall 2004).
Id.
Id.
Michelle Alexander, supra note 27.
Id.
Id.
Michael Tonry, Malign Neglect – Race Crime and Punishment in America 82 (London: Oxford University Press, 1995).
Is Addiction a Disease, P’ship to End Addiction, (Mar. 2023) www.drugfree.org/isaddictionadisease.
Id.
Id.
Id.
Research Reports, National Institute on Drug Abuse nida.nih.gov/publications/research-reports/.
Is Addiction a Disease, Partnership to End Addiction, (Mar. 2023) www.drugfree.org/isaddictionadisease/.
Id.
Drug Addiction (Substance Abuse Disorder), Mayo Clinic (Oct. 4, 2022), http//www.mayoclinic.org/ diseases-conditions/drug-addiction/symptoms-causes/syc-20365112.
Id.
Id.
Is Addiction a Disease, supra note 54.
Id.
Is Addiction a Disease, supra note 54.
Is Addiction a Disease, supra note 54?
Krystina Murray, Sugar Addiction, Addiction Ctr., (Nov. 6, 2019), http//www.addictioncenter.com/sugaraddiction/.
Center on Addiction, Behind Bars II: Substance Abuse and America’s Prison Population, (Feb. 2010), https://eric.ed.gov/?id=ED509000.
Id.
Criminal Justice DrugFacts, Nat’l Inst. on Drug Abuse (June 2020) nida.nih.gov/publications/drugfacts/criminal-justice.
Ingrid A. Binswanger et al., Release from Prison—A High Risk of Death for Former Inmates, 2 New England J. of Med. 356, 157–65, 161 (2007).
Id.
Shabbar I. Ranapurwala et al., Opioid Overdose Mortality Among Former North Carolina Inmates: 2000–2015, 9 Am. J. of Pub. Health 108, 1207, 1207–13, (2018).
Id.
dep’t of rsch. and acad. engagement, (Mar. 2023) http//www.drugpolicy.org/research.
Id.
leading addiction treatment centre, (Mar. 2023) www.oceanrecoverycentre.com.
Id.
Glen Greenwald, Drug Decriminalization in Portugal: Lessons for Creating Fair and Successful Drug Policies.
Id.
Glen Greenwald, Drug Decriminalization in Portugal: Lessons for Creating Fair and Successful Drug Policies, U.S. Dep’t of Just.: Off. Of Just. Prog. (2009), https://www.ojp.gov/ncjrs/virtual-library/abstracts/drug-decriminalization-portugal-lessons-creating-fair-and-0.
Instituto da Droga e da Toxicodependência de Portugal, pamphlet intended for public consumption by the citizenry, https://www.emcdda.europa.eu/system/files/publications/.
The Four-Pillar Policy, Fed. Off. of Pub. Health (last modified July, 5, 2021), http//www.bag.admin.ch/bag/en/home/strategie-und-politik/politische-auftraege-und-aktionsplaene/drogenpolitik/vier-saeulen-politik.html.
Id.
Id.
Id.
Id.
Id.
Id.
Id.
Id.
Taylor Knopf, Switzerland couldn’t stop drug users. So it started supporting them, N.C. Health News (Jan. 21, 2019), https://www.northcarolinahealthnews.org/2019/01/21/.
Id.
Id.
Id.
Chris Roberts, Oregon Legalizes Psilocybin Mushrooms and Decriminalizes All Drugs, Forbes (Nov. 4, 2020), https://www.forbes.com/sites/chrisroberts/2020/11/04/oregon-legalizes-psilocybin-mushrooms-and-decriminalizes-all-drugs/?sh=3d99c40a4b51.
Alexandra Harrison, Oregon Decriminalizes Drugs, Replaces Arrests With Health Care, Reason Found. (Feb. 23, 2021), https://reason.org/commentary/oregons-decriminalizes-drugs-replaces-arrests-with-health-care/.
Id.
Id.
transform drug policy foundation, (Mar. 4, 2023), http//www.transformdrugs.org.
Council of Europe (2001-2019), Space Project: Annual Reports 2001-2019, https://wp.unil.ch/space/space-i/annual-reports/.
Decriminalization vs Legalization of Drugs: What It Means For States in 2020-2021, Turnbridge, http//www.turnbridge.com/decriminalization-vs-legalization/.
Id.
Id.
Id.